
You’ve tried the painkillers. You’ve adjusted your pillow, cut back on caffeine, and tracked your sleep. The headaches keep coming back anyway, always starting in the same spot, always following the same pattern.
Here’s what most people don’t realise. A significant portion of chronic headaches don’t originate in the head at all. They start in the neck, specifically in the joints and muscles of the upper cervical spine, and travel upward through shared nerve pathways. The pain lands in your head, but the source is somewhere else entirely.
If you’ve been told you have migraines but the diagnosis never quite felt right, or the treatment hasn’t delivered lasting relief, it’s worth considering whether your neck is actually the problem. Cervicogenic headache affects between 15 and 20% of people with chronic headaches and is one of the most frequently misdiagnosed conditions in physiotherapy. Most people get labelled with tension headaches or migraines, take medication that partially works, and spend months wondering why nothing sticks. This guide breaks down the five signs that your neck is driving your headaches, what’s actually happening underneath, and how to properly address it.
What Cervicogenic Headache Actually Is
Cervicogenic headache is a secondary headache caused by an underlying disorder in the neck, such as joint, disc, or nerve irritation. The pain doesn’t start in your head. It starts in your neck and travels upward through shared nerve pathways, landing across your forehead, behind your eye, or at your temple.
Many people assume this kind of pain is a migraine because of where they feel it. But unlike a migraine, the trigger isn’t neurological. It’s structural, and that distinction changes everything about how it should be treated.
This is why it responds so poorly to standard headache medication. Painkillers work on the signal. They can’t touch the stiff joint or the overworked muscle that’s generating it
Why It Gets Missed So Often
Around 47% of the global population experiences regular headaches. Of those with persistent or recurring symptoms, 15 to 20% have cervicogenic headache as the real underlying cause. In people who’ve had a whiplash injury, that figure climbs to 53%.

It tends to show up most in people aged 30 to 44, and while women are significantly more likely to be diagnosed with it in a clinical setting, the condition affects men and women fairly equally in the wider population.
On the surface, it looks like a migraine or tension headache. The pain is real; it’s in your head, and medication takes the edge off temporarily. So it gets labelled and managed accordingly and never actually resolved. Getting the right diagnosis changes everything. Once the neck is identified as the driver, the focus shifts to fixing the cause rather than quieting the symptom.
5 Signs Your Headache Is Coming from Your Neck
Sign 1: The Pain Consistently Starts at the Base of Your Skull
Cervicogenic headache begins at the back of the head, right where the neck meets the skull, and spreads forward toward the forehead, eye, or temple. The pattern is predictable and repeatable. Unlike migraines, which often come with visual disturbances or nausea, or tension headaches that wrap around the whole head, a cervicogenic headache has a fixed point of origin you can usually press on and recognise immediately.
Sign 2: It Stays on the Same Side Every Time
Cervicogenic headache affects one side of the head and stays there, regardless of how long it lasts or how intense it gets. Migraines can shift sides over multiple episodes, but cervicogenic headache doesn’t. If your headaches are reliably on the same side every time, that’s a strong indicator that a specific structure on that side of your neck is responsible. Research puts one particular joint in the upper neck at the root of 50 to 70% of cases.
Sign 3: Neck Movement or Sustained Posture Triggers It
If turning your head, looking up, or sitting in the same position for a long time reliably brings on or worsens your headache, the neck is involved. Migraines are typically triggered by things like hormones, certain foods, or sleep disruption, not by checking your blind spot or looking down at your phone. Think about your patterns. Does it build after a long stretch at your desk? Does it spike when you cough or sneeze? Does reversing the car set it off? If more than one of these sounds familiar, your neck is most likely the trigger.
Sign 4: Your Neck Is Stiff, or Your Range of Motion Is Limited
Most people with cervicogenic headaches have noticeably reduced neck movement, especially when rotating to one side. You might find it harder to check your blind spot, or your neck might feel locked up, first thing in the morning. The stiffness and the headache aren’t two separate problems. They’re two expressions of the same one.
Sign 5: Pressing on Your Neck Reproduces the Headache
If a physiotherapist applies pressure to specific points in your upper neck and it reproduces the exact headache you’ve been experiencing, that confirms where the problem is coming from. It cuts through the guesswork. When you can point to the structure causing the pain, treatment becomes precise rather than general.
How Does Your Headache Compare?
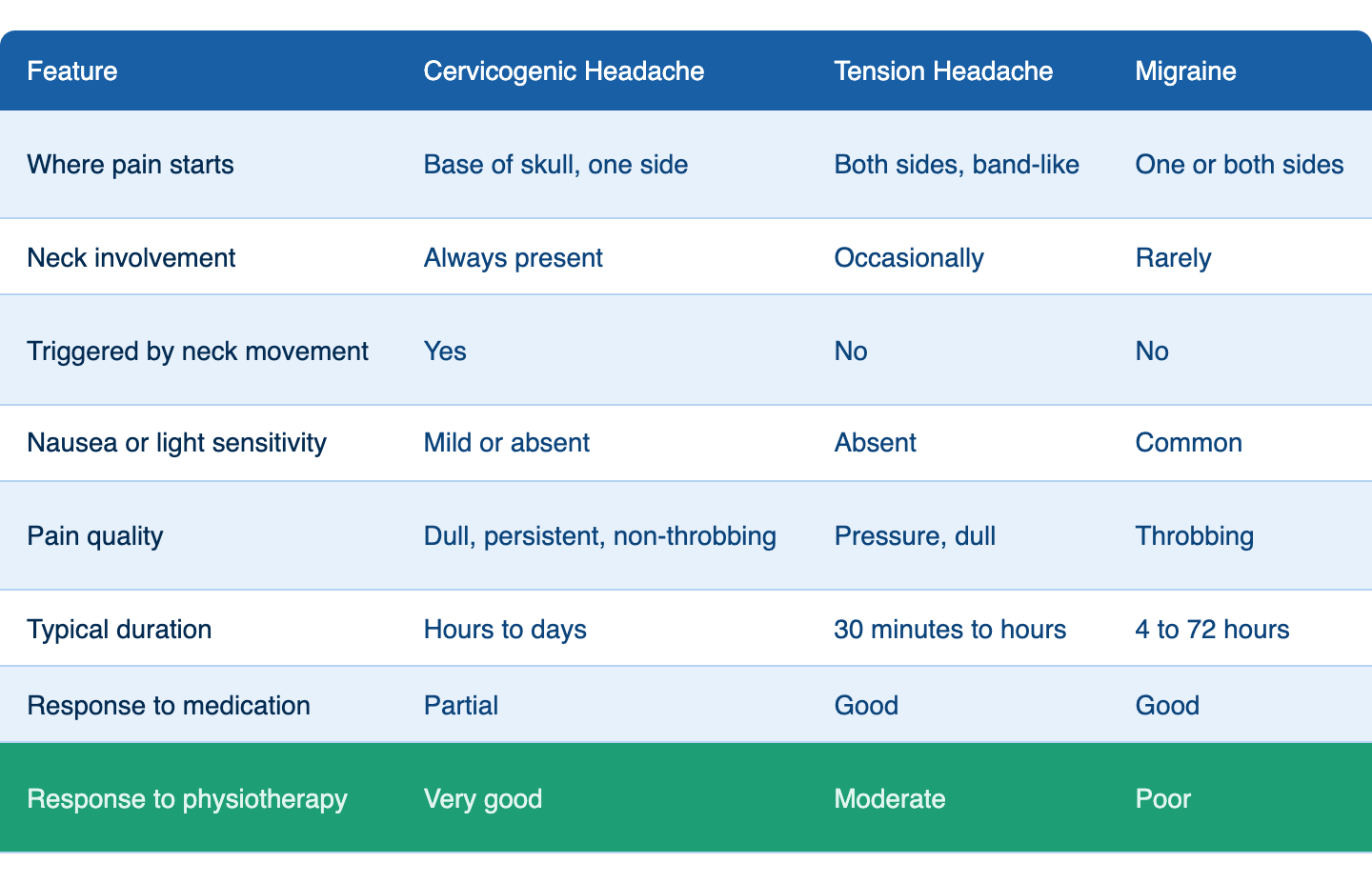
If your headaches respond only partially to medication and keep returning despite consistent treatment, that pattern is itself diagnostic. A cervicogenic headache is a structural problem, and structure responds to structural treatment.
What the Research and Medical Community Say
Cervicogenic headache is a well-established condition in medical literature, recognised by institutions including the National Institutes of Health and major clinical bodies worldwide. It’s defined as a secondary headache caused by an underlying disorder in the neck, involving the joints, discs, or nerves of the cervical spine.

At Mickleham Physiotherapy, we assess and treat this condition regularly. The clinical picture described in the research lines up directly with what we see in our patients every week. One-sided pain starting in the neck, stiffness, restricted movement, and a history of partial or no response to standard headache medication. Getting a proper hands-on assessment is what turns that clinical picture into a clear diagnosis and a treatment plan that actually works.
What’s Driving It
The most common culprits are joints in the upper neck that have become stiff or restricted, tight muscles at the base of the skull that are working overtime, the kind of forward head posture that builds up from long hours at a desk or on your phone, and old neck injuries like whiplash that may have seemed minor at the time but left lasting stiffness behind.
One specific joint in the upper neck, where the second and third vertebrae meet, tends to be the most frequent source of trouble. Research puts it at the root of somewhere between 50 and 70% of cervicogenic headache cases, and even more so in people who’ve had a whiplash injury. In those patients, physiotherapy has been shown to produce lasting improvements in both neck movement and headache frequency. When the neck is the problem, treating the neck is what works.
How We Treat It at Mickleham Physiotherapy
Structured assessment. Before anything else, we assess how your neck moves, feel for joint restrictions and tender spots, and use specific tests to pinpoint which structure is responsible. This is targeted, not a general once-over.
Hands-on joint work. Manual therapy applied to the restricted joint is the most evidence-supported treatment for cervicogenic headache. Restoring normal movement reduces the irritation generating referred pain in your head.
Muscle work. Tight muscles at the base of your skull and across your upper neck and shoulders often feed the problem. Dry needling and soft tissue therapy release the specific spots that reproduce your headache.
Postural correction. If forward head posture is loading your upper neck all day, that needs to change, or the headaches will keep coming back. We look at how you sit, work, and move, and make adjustments that fit your actual life.
Progressive exercise. Strengthening the muscles that support your neck reduces ongoing strain on the joints, driving your headache. These exercises become part of your routine so the results last well beyond the treatment room.

Frequently Asked Questions
How do I tell the difference between a cervicogenic headache and a migraine?
Cervicogenic headache starts at the base of the skull, stays on one side, and gets worse with neck movement. Migraines typically come with nausea, light sensitivity, and a throbbing quality. We can assess your neck and determine fairly quickly whether it’s the source.
Can physiotherapy resolve it permanently?
For most patients, yes. When the problem is a restricted joint, overloaded muscles, or poor posture, addressing those things properly produces lasting results. Completing the full treatment plan, including the exercises, is what separates short-term relief from lasting resolution.
Why hasn’t medication worked for me?
Because medication addresses the pain signal, not the structure producing it. If a restricted joint in your neck is generating that signal, pain relief will dampen it temporarily but won’t change the underlying mechanics. That’s why physiotherapy, which targets the cervical spine directly, is what actually works.
We See This Every Day at Mickleham Physiotherapy
Persistent headaches that don’t respond to medication, keep returning on the same side, and seem to follow neck movement or posture are telling you something. The source is most likely structural, and the structure is most likely your neck.
At Mickleham Physiotherapy Services, we carry out thorough, hands-on cervical assessments to identify where your headaches are actually coming from, not just manage the symptoms. Our team in Melbourne’s northern suburbs works with patients dealing with exactly this kind of persistent, misdiagnosed pain every week. Whether you’ve been living with this for months or years, a proper assessment is where real progress begins.
Contact us and let us find out what’s actually driving your headaches. You don’t have to keep managing something that can actually be fixed.